


1Department of Dermatology and Allergy, Herlev and Gentofte Hospital, University of Copenhagen, and 2Copenhagen Research Group for Inflammatory Skin, Herlev and Gentofte Hospital, DK-2900 Hellerup, Denmark. E-mail: nikolai.dyrberg.loft@regionh.dk
Accepted Aug 8, 2019; E-published Aug 9, 2019
In recent years, administrative registry data has been used with increasing frequency in dermato-epidemiological studies (1, 2). A common approach to the identification of patients is through use of the International Classification of Diseases, 10th revision (ICD-10) codes (2–4). This study aimed to validate the diagnostic code for psoriasis (ICD-10 L40.0) recorded in the Danish National Patient Register (5).
The study was approved by the Danish Data Agency (ref. 2012-58-0004, j.no. VD-2018-286, I-Suite no.: 6528) and the Danish Patient Safety Authority (j.no. 3-3013-2654/1, ref. EMGW).
From among all patients seen in our department (the Department of Dermatology and Allergy, Herlev and Gentofte Hospital, Hellerup, Denmark), we randomly selected 100 adults and all children with a recorded diagnosis of psoriasis vulgaris in the National Patient Register ICD-10 code L40.0 between 1 January 2008 and 23 October 2018. In case of multiple diagnoses of psoriasis during this period, the first of these was used as the index date. The criterion for validity was the use of terms consistent with psoriasis vulgaris with no other competing dermatological diagnosis (e.g. dermatitis or pustular psoriasis) in the patient’s medical chart on the same date that the diagnosis was recorded. Data extracted from the chart included age at recorded diagnosis, age of psoriasis onset, sex, psoriasis type, Dermatology Life Quality Index (DLQI), body surface area (BSA), Psoriasis Area Severity Index (PASI), location, potential triggers, first location, and familiar disposition.
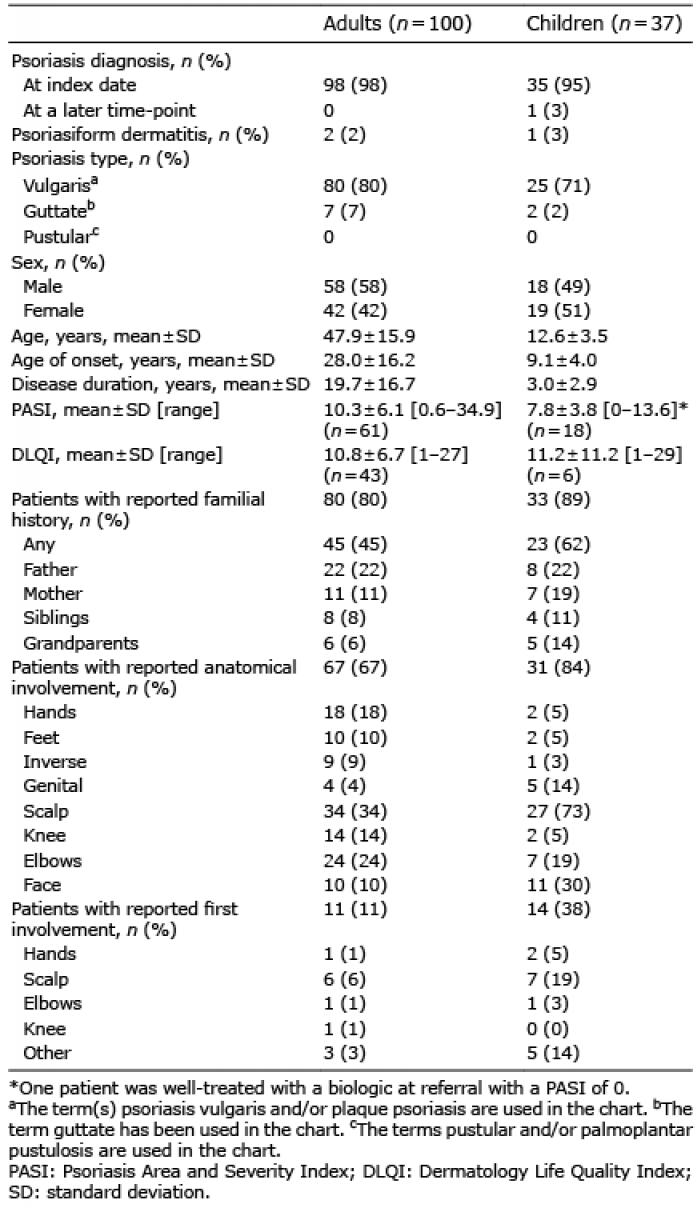
The study comprised a total of 137 patients, of whom 100 were adults and 37 were children (Table I). Few patients had an identified trigger (n = 3), and BSA was reported in only 2 patients. The psoriasis diagnosis could not be verified in a total of 4 patients, 2 adults and 2 children, from the medical chart on the same date as the diagnosis was recorded. In the medical chart 1 of the 2 children was noted to definitively have psoriasis on a later date, whereas the 3 remaining patients were reported to have psoriasiform dermatitis. Consequently, the overall positive predictive value (PPV) of the study was 97.1% (95% confidence interval (95% CI) 95.5–98.1). In adults, the PPV was 98.0% (95% CI 95.7–99.1), and in children the PPV was 94.6% (95% CI 88.7–97.5).
Table I. Clinical and demographic characteristics of patients with L40 diagnosis
This study found a high PPV of the ICD-10 code for psoriasis in the Danish National Patient register. Recently, a medical chart review found a similarly high PPV for diagnosis of atopic dermatitis in the same register (6). This demonstrates consistency in the use of ICD-10 codes in skin diseases in Denmark. However, as diagnoses were made by a dermatologist, the validity of diagnoses from other departments, e.g. emergency departments, might not be similar. Nevertheless, the given estimate of the PPV is considered conservative, as only patients with the diagnosis on the index date were included as cases.
The observed mean PASI corresponds to moderate-to-severe psoriasis (7) consistent with that seen in patients receiving systemic (mean±standard deviation (SD), PASI of 8.3 ± 6.4) (8) and biologics (PASI of 13.2 ± 8.1) (9), which is consistent with this being the first time most of the patients were seen in a university hospital. However, the recorded PASI ranged from negligible to very severe disease, which might be attributed to the fact that some patients were already receiving systemic treatments at referral. The high proportion of children with a familial history of psoriasis is consistent with type 1 psoriasis showing a strong genetic predisposition (10).
This study was limited by the single-centre design; however, since all hospital dermatology departments in Denmark are academic university departments, we suspect that similar findings would apply at other departments in the country.
In summary, this study suggests that the use of the ICD-10 code L40.0 to identify patients with psoriasis is a valid approach in registry-based studies.
Funding and conflicts of interests. NDL has been an honorary speaker for Eli Lilly. AE has received research funding from Pfizer, Eli Lilly, the Danish National Psoriasis Foundation, and the Kgl Hofbundtmager Aage Bang Foundation, and honoraria as consultant and/or speaker from AbbVie, Almirall, Bristol-Meyers Squibb, Leo Pharma, Samsung Bioepis Co., Ltd, Pfizer, Eli Lilly, Novartis, Galderma, and Janssen Pharmaceuticals. JPT has attended advisory boards for Sanofi-Genzyme, Union Therapeutics and Eli Lilly & Co, and received speaker honorarium from LEO Pharma and Sanofi-Genzyme, and been an investigator for Sanofi-Genzyme, Eli Lilly & Co, LEO Pharma and Abbvie. LS has received speaker honoraria from Abbvie, Pfizer, Janssen-Cilag, and Leo Pharma and is a member of the advisory boards of Abbvie, Pfizer, Janssen-Cilag, Sanofi, Eli Lilly, Celgene and Novartis. CA and ASHO report no conflicts of interest.


 Click to show fullsize
Click to show fullsize